
Anterior Knee Pain
What are the causes?
Anterior knee pain generally describes pain arising from the kneecap (patella) or the surrounding structures around it. For the purposes of this section we will talk about “patellofemoral pain syndrome” also commonly known as “chondromalacia patella”.
For completeness, other causes of anterior knee pain include:
What is
Patellofemoral pain syndrome?
Patellofemoral pain syndrome is a condition that causes pain that is arising from the patella that is not due to one of the above causes of anterior knee pain.
It is generally caused by either

Is patellofemoral pain syndrome common?
Patellofemoral pain syndrome is very common.
It can affect patients in their teenage years as well as those in the 30-40 year age group.
It more commonly affects females as compared to males.
What are the symptoms ofPatellofemoral pain syndrome?
Tipically the pain is worse with activities that place load on the knee when it is bent (flexed). For example:
The pain tends to be better with activities on level ground when the knee is much less bent.
Classically the pain is around or directly under the kneecap. It can vary from a dull ache to a sharp stabbing character.
The pain is not usually associated with much swelling
Often the patient experiences a sensation of grinding or grating from the kneecap
What causes
Patellofemoral pain syndrome?
The two common causes are overuse and patella malalignment. The two can coexist.
Patella malalignment
This condition is more common in women. Due to anatomical factors, the kneecap may not align properly in the groove on the front of the thigh bone. It can be tilted, shifted sideways, or positioned too high.
Patella Overuse
This can be caused after commencing a new physical activity that involves repetitive lunging, squatting and up and down stairs.
Other related anomalies can include being “knock kneed” or “pigeon toed”, both of which can contribute to a maltracking kneecap.
Can I have a maltracking kneecap and have no problems?
Yes you can.
I often see patients with pain only in one knee but on examination they have kneecap maltracking in both knees.
How do you diagnose
Patellofemoral pain syndrome
The condition is diagnosed through a combination of:

A classic history with location of pain and exacerbating factors

Signs of maltracking on examination and investigations
What investigations should I have?
The diagnosis can be made on history and examination alone.
In patients with a long history or recurring symptoms or in whom non surgical treatments have not helped the following investigations can be useful

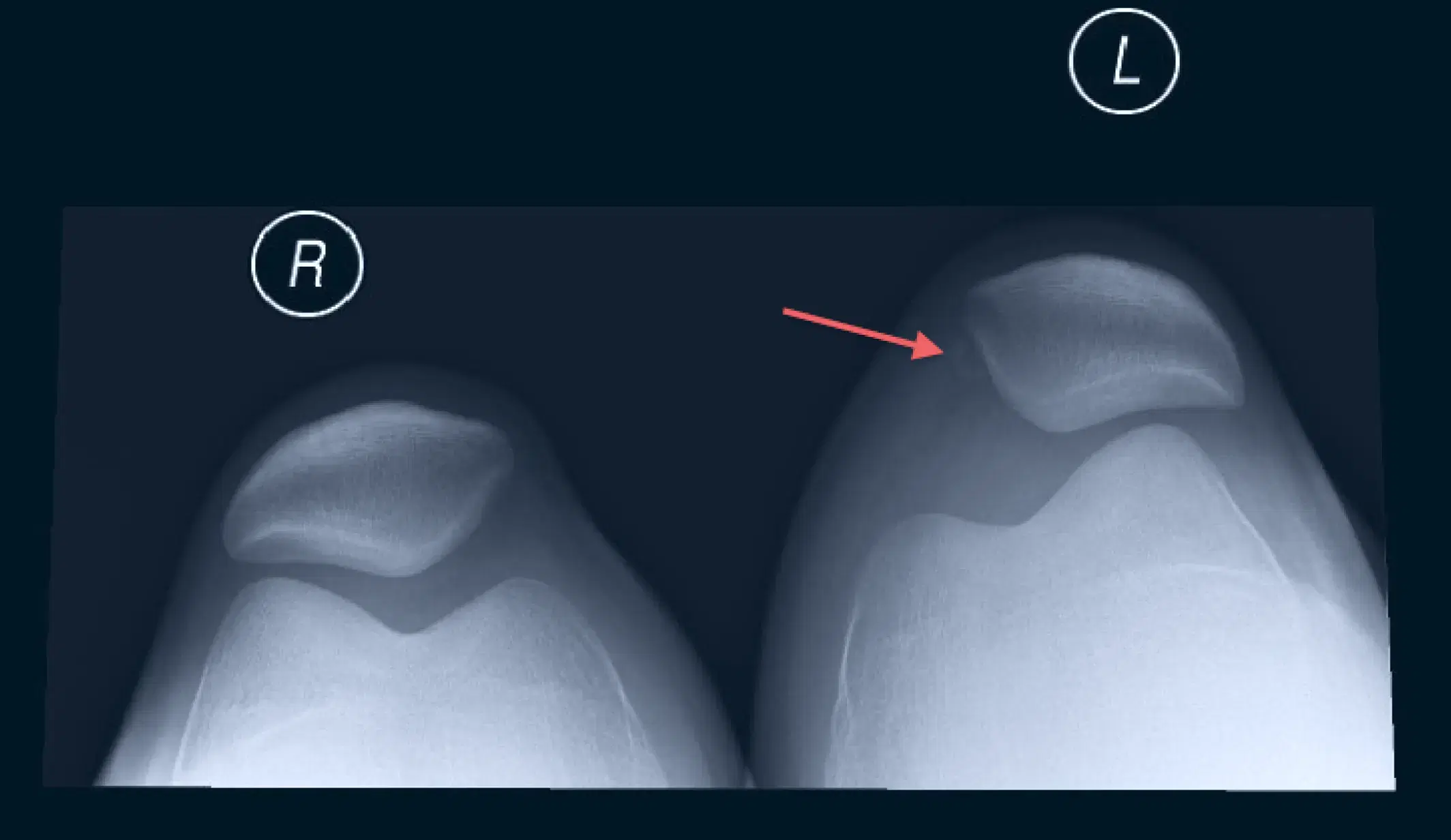
X-rays
Including special views of the kneecap to look for signs or maltracking or arthritis


MRI scan
An MRI scan to look at the quality of the cartilage underneath the kneecap as well as signs of maltracking
What investigations
should I have?
The diagnosis can be made on history and examination alone.
The majority of patients improve with



A trial of kneecap taping if there are signs of maltracking

Patella toping
What does
Physiotherapy do?

Physiotherapy is very important in the treatment of this condition.
The physiotherapist can work on strengthening the muscles on the front of your thigh (quadriceps), stretch the muscles and tendons on the side and back of your thigh (hamstrings), as well as give you exercises to have better control of your musculature.
Is an arthroscopy useful in the treatment of this condition?
An arthroscopy has limited usefulness in the treatment of this condition.

Do you need a
Knee replacement?
Dr Seeto in affiliation with Medibank Private and East Sydney Private hospital, offers a program for eligible Medibank Private Members, to eliminate medical out of pocket costs for your Knee Replacement.
The program includes a pre-surgery preparation program, spending the minimal time necessary in hospital, as well as home rehabilitation if necessary.

Book a consultation
today
9:00 am - 4:30 pm